
Last week, Mariska Bot and colleagues published a clinical trial in JAMA whereby they randomized overweight or obese adults with subsyndromal depressive symptoms to placebo, micronutrients (400 mcg folic acid, 800IU vitamin D, 30 mcg selenium, 100 mg calcium, and 1412 mg DHA+EPA), micronutrients plus behavioural activation or placebo plus behavioural activation. Their primary outcome was cumulative onset of an episode of Major Depressive Disorder (MDD).
Their press release held this title: “Nutritional supplements cannot prevent depression”. The media reports on the study generally concluded that a handpicked cocktail of nutrients cannot prevent depression before it strikes: Healthy Living not a panacea for depression, No, nutritional supplement pills don’t help people fight depression, and Multivitamins do not help stave off depression but lifestyle coaching may work. One would assume that people got worse as part of participation in the trial.
This was not the case.
Let’s look at the data.
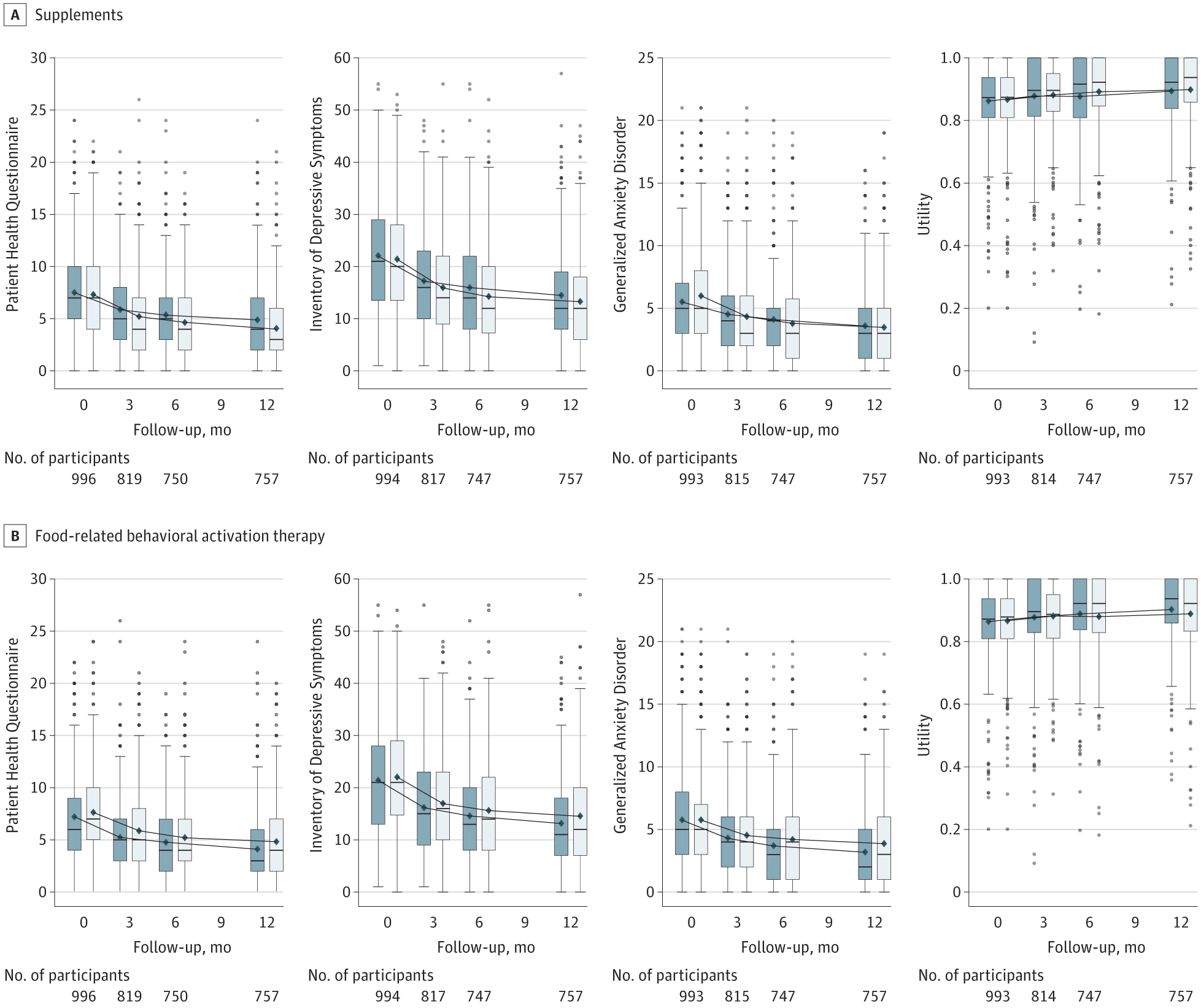
The graphs (Figure 2) provided by the researchers showed, on average, all groups got better over time based on measures of depression, anxiety, and health status. They also provided statistics to show that there were significant group differences pre to post intervention. In other words, those taking the nutrients were significantly better at 12 months compared to how they were at baseline.
So why did the researchers report in the discussion that nutrients “showed no effect”? What they should have said was that all groups got better over time, but there were no group differences in the prevention rates of MDD. I can’t believe that this inaccuracy in reporting got through extensive review by this journal, one of the best in medicine.
However, despite the overall mean going down, a small percentage of the entire sample got worse, with on average 10% meeting criteria for MDD by 12 months with no group differences among the different interventions: 25 (9.7%) patients in the placebo without therapy, 26 (10.2%) in the placebo with therapy, 32 (12.5%) in the supplement without therapy, and 22 (8.6%) in the supplement with therapy group.
Interestingly, this rate of conversion was half of what the researchers expected, which actually means participating in a clinical trial will help stave off depression, regardless of the group you get randomized to. What a good news story. Interesting that the headlines didn’t focus on the behavioural activation therapy not working even though it was no better than the nutrients.
Why were only the nutrients singled out in the headlines?
One has to ask, was their handpicked cocktail of nutrients a reasonable choice? Based on 10 years of studying the effects of micronutrients, I would say absolutely not. Researchers who work in this space hypothesize that the body needs a full blend of nutrients in order for the brain to function optimally – this means the full range of vitamins and minerals. The JAMA study provided 2 vitamins and 2 minerals, all below Recommended Daily Allowances (RDA). Research from my lab, the Mental Health and Nutrition Research Group at the University of Canterbury, has shown that a micronutrient formula containing 12 vitamins and 16 minerals, typically at doses higher than RDA, was significantly more effective in reducing moderate to severe symptoms of depression as compared with people taking the placebo. Other researchers have shown similar positive effects of nutrients on MDD. We, with others, have written about the importance of providing the full range of nutrients in order to give the body the best chance of recovering from mental illness, to combat oxidative stress and inflammation, and improve the functioning of the microbiome and mitochondria. Our current studies are designed with this in mind. Buyer beware. Not all “nutritional supplements” are equal.
Let’s look at another trial investigating the prevention of recurrence of MDD with either mindfulness-based cognitive therapy (MBCT) or cognitive therapy (CT) published just last year. This trial was not that different from the Bot et al. trial in terms of the goal of the study. After 2 years, 21% of those randomized to MBCT had relapsed versus 22% of those randomized to CT. No group differences. But the headlines weren’t that the treatments had failed, but rather that “both interventions (were) equally effective”. The media headlines reflected the overall benefit of these interventions: MBCT and cognitive therapy equally effective for depression relapse. Quite the contrast to these recent headlines deploring the efficacy of nutrients.
Poor reporting happens in the antidepressant literature as well. Headlines like “antidepressants don’t work” are usually not accurate and only serve to create divisions. Antidepressants do work in terms of people showing a lowering of symptoms of depression over time in clinical trials; however, often times the improvement is not that much different than the improvement observed in the placebo group. In other words, antidepressants can reduce symptoms of depression in the short-term but not clinically significantly more than placebo and longer-term efficacy has not been established. Indeed, many of these trials reveal the power of nonspecific effects in healing.
No wonder the public are confused when trials are not accurately reported both in the scientific articles and then in the media reports.
Sadly, the reporting of the JAMA trial has been misleading, confusing and overall the trial was not adequately designed to answer the question about whether nutritional supplements work to prevent depression. That trial cost the European tax payers millions of Euros to run. You would have thought they would get it right from the start.
Scientists and journalists, let’s work together to help improve accuracy in reporting of clinical trials. We owe it to the public to not let our inherent biases misrepresent the data.
Julia Rucklidge is a Professor of Clinical Psychology in UC’s Department of Psychology and the Director of the Mental Health and Nutrition Research Group.




")






{kind=link}
{kind=link}